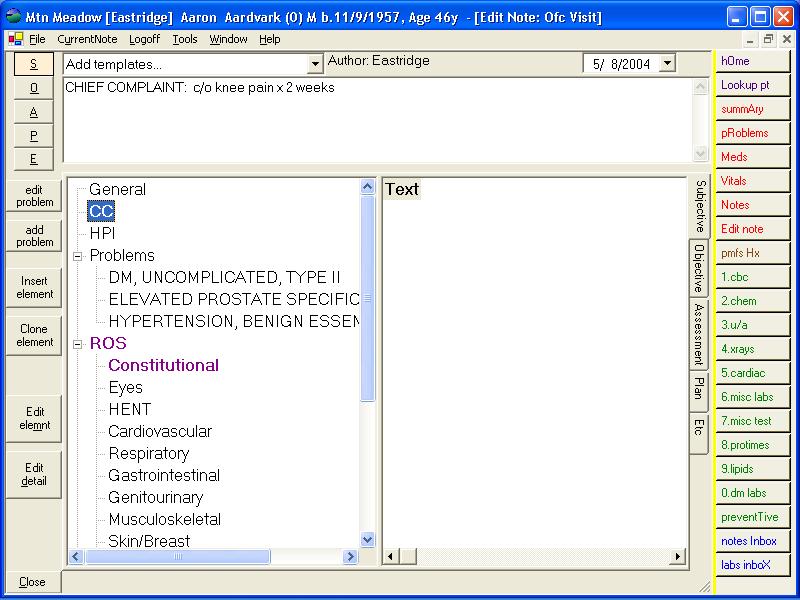
To begin a patient encounter, the nurse will log in and begin a new note. Typically they will enter the reason for the visit under "Chief Complaint."
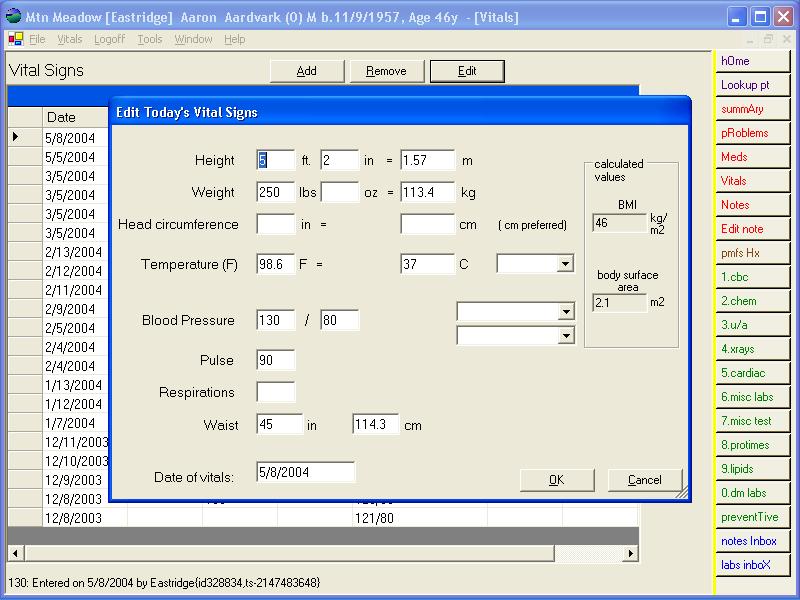
Next, they will enter vital signs.
Finally, they will look in the Preventive section to see if the patient is due any preventive medicine interventions.
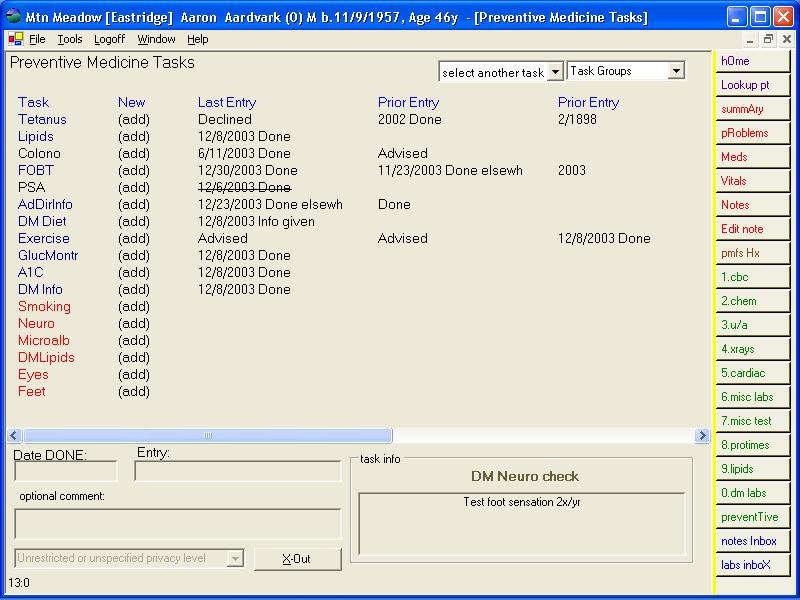
Red colored interventions are due. The nurse will schedule or do the required intervention and click (add) to document it, or to document if the patient declined to have it done.
Then the nurse will log off.
The doctor will log in upon arrival and see the chief complaint. They may choose to type in details about the history as they interview the patient. Alternatively, they may choose to dictate it later to be typed in by a transcriptionist or by a voice recognition program such as Dragon Naturally Speaking.
Most of the physical exam can be entered quickly by clicking selections in the branching trees of the note generator.
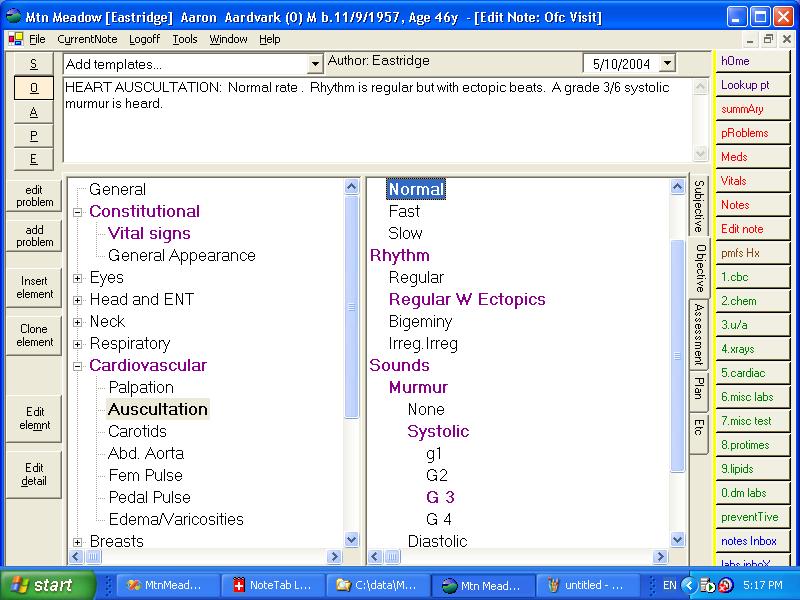
The clinician may edit elements of the note that differ from the choices in the template. Furthermore, they may choose to add those amendments to the template for future use.
The doctor or nurse may refil prescriptions simply by double clicking on them, and clicking "Print." New prescriptions can be written by typing in free text or choosing from a list of medicines that are available.
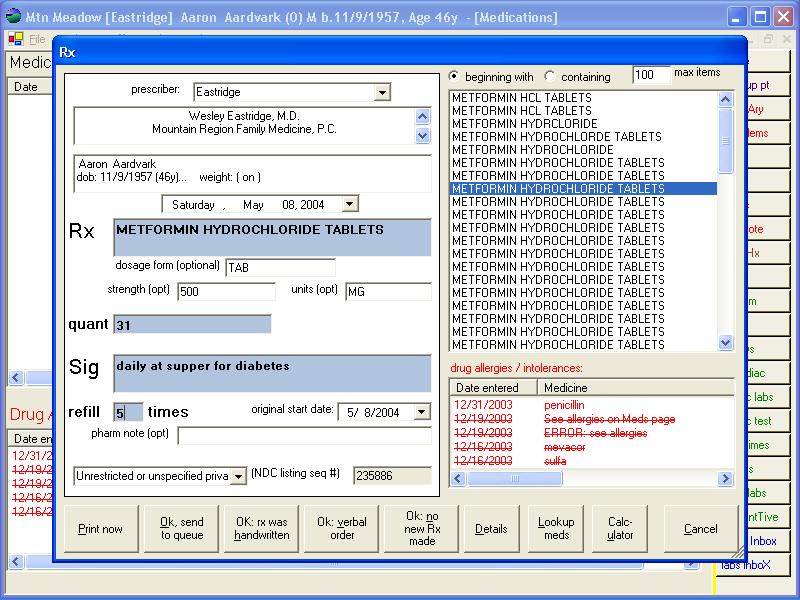
The drug allergies are shown on the page as the prescription is written to help avoid prescribing drugs the patient is allergic to.
Future enhancements will incorporate a third-party database to check for drug interactions and allergies automatically.
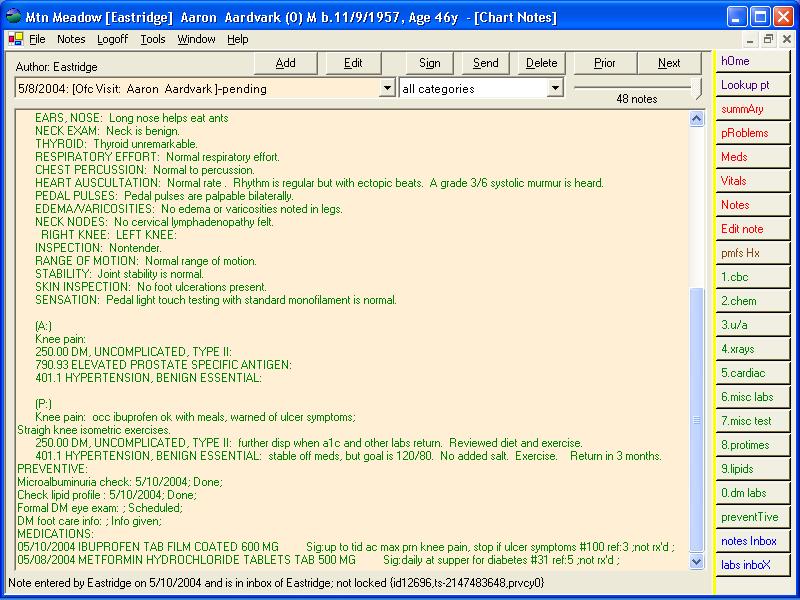
When the office encounter is finished, the chart note is already generated. A copy can be printed for a consulting physician. The patient may receive a copy of the whole note, or just special instructions or the medication list if desired.